




Introduction
From 2019, the European Societies for Cardio-Thoracic Surgery (European Association for Cardio-Thoracic Surgery – EACTS) and Vascular Surgery (European Society for Vascular Surgery – ESVS) recommend the setting up of so-called “Aortic Teams” to effectively treat aortic arch pathologies both openly and endovascularly. It is recommended to centralise treatment in centres treating both methods simultaneously (recommendation class 1C) [1]. So practically, this means that Aortic Teams should operate within cardiac surgery departments. They should be equipped with hybrid rooms and employ both cardiac surgeons and vascular surgeons.
Material and methods
In July 2021, the first Polish “Aortic Team” operating within cardiac surgery was officially established in Szczecin. This legalised the long-standing cooperation between Szczecin’s “vascularists” and cardiac surgeons (starting in 2018). At the moment the Aortic Team consists of one cardiac surgeon, two vascular surgeons, two cardiologists, one anaesthesiologist and one coordinator.
Sixty-four patients were treated as part of the Aortic Team (since the beginning of cooperation). Patients with aortic arch pathology not directly eligible for open treatment with the frozen elephant trunk (FET) technique (high-risk patients) were first qualified for treatment with custom (patient tailored) stent grafts. If patients were disqualified by the manufacturer due to anatomical contraindications, e.g. inadequate aortic diameter, mechanical valve, “kinking”, coronary bypasses, they were qualified for treatment with stent grafts modified by the physician. If this too was not possible or safe, patients were re-qualified for less durable thoracic endovascular aortic repair (TEVAR) plus procedures (see below), re-qualified for FET or disqualified from surgical treatment altogether.
Results
There were 64 procedures performed with a technical success rate of 91% and 11% bad outcomes (deaths and strokes). A good outcome was achieved in a total of 89% of patients.
Among the aortic arch procedures, the team performed 19 TEVAR plus procedures (due to the need for proximal landing in zones 0 to 3 according to Ishimaru) [1]. This group included patients who underwent TEVAR with an additional procedure (chimneys/periscopes, n = 7, extraanatomical bypasses of arteries diverging from the aortic arch, n = 12) with 100% technical success and 4% bad outcomes (stroke or death). There were also 12 implantations of “customized” stent grafts into the aortic arch including Bolton Relay plus Custom Made Devices double/triple-branch endoprosthesis (Bolton Medical, Sunrise, FL, USA), n = 8, Brail Endo-Branch System (Biomedica, Italy), n = 1, and Castor branched aortic stent graft (MicroPort Endovascular MedTech Co., Ltd. Shanghai), n = 3, with 91% technical success and 18% bad outcomes. As the only team in Poland we performed 30 implantations of physician-modified endo-grafts (PMEG) based on the Valiant thoracic platform (Medtronic, USA) in 14 cases with one fenestration to the subclavian artery (LSA), in 5 cases with fenestration to two arteries (LSA and left common carotid artery) and 11 cases with triple fenestration to all vessels of the aortic arch – including an additional coronary bypass window in 1 case. In this group, technical success was achieved in 91% and poor outcome ended treatment in 11%. In the group of patients treated endovascularly, externalized transapical guidewire (ETAG) technique was used in 16 cases, resulting in 100% technical success in the group of patients treated with PMEG technique (statistically insignificant difference, 60% vs. 100%; p = 0.51). In the group of patients treated with open technique (n = 3), FET was performed, recording 33% bad results (group not yet representative due to insufficient size).
In the group of patients treated endovascularly, the Aortic Team used the following novel techniques: it was the first in the world to successfully use the modified ETAG technique in a patient with an artificial aortic valve (n = 4) [2]. It was one of the first in the world to use 3D printing and holography to prepare and perform PMEG procedures in both the aortic arch and thoracoabdominal segments [3–5]. It also successfully treated patients with type A dissection in stages using the novel e-provisional extension to induce complete attachment (e-PETTICOAT) method [6]. It also introduced a new technique of modifying stent grafts intended for the treatment of arch pathologies by using a double parallel reefing of the stent graft [7] (Figure 1).
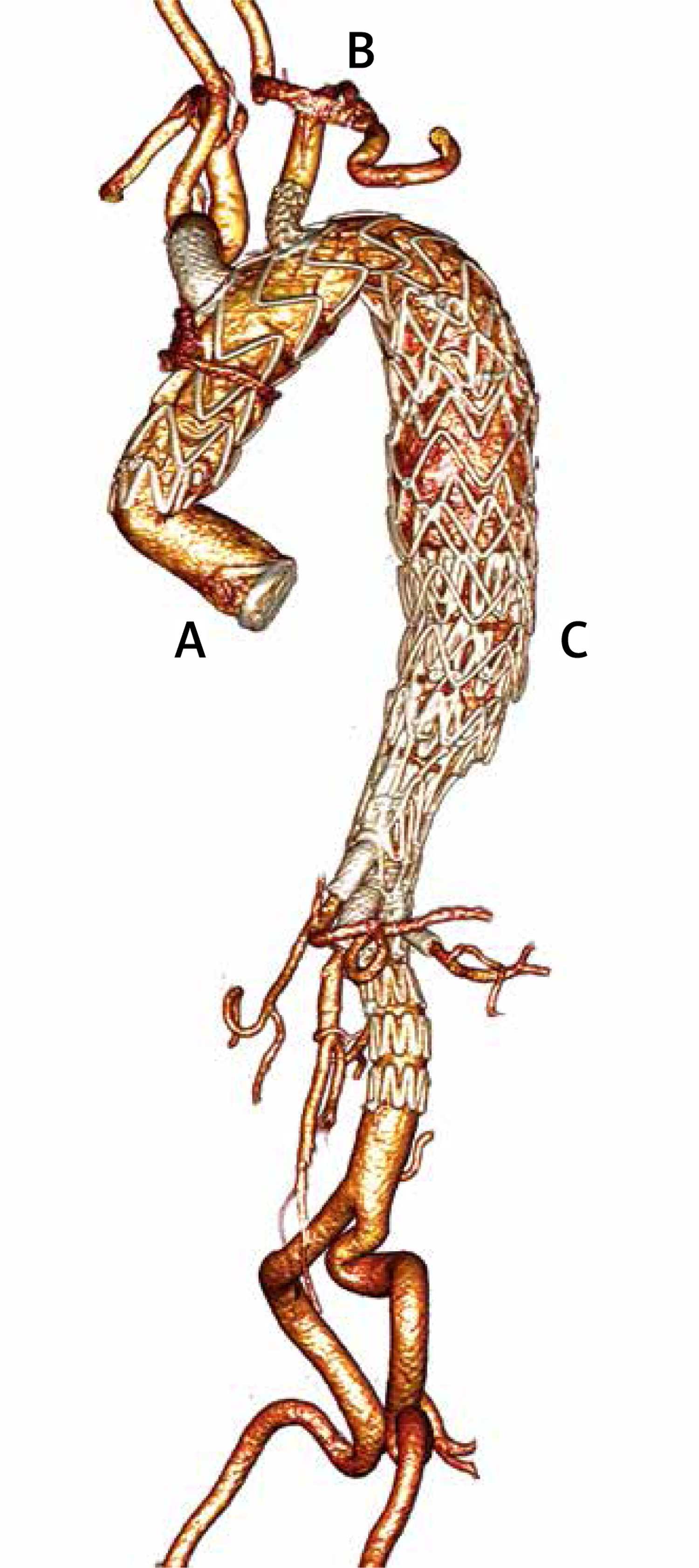
Figure 1
Example images of aortic arch after endovascular treatment with PMEG: A – single fenestrae to LSA, B – double fenestrae to LSA and LCCA, C – triple fenestrae to LSA, LCCA and IA, D – quadruple fenestrae to LSA, LCCA and IA and for coronary bypass

In the group of patients treated with the open technique, our team made some changes to the standard surgical technique. We introduced an obligatory oversizing (by at least 2 mm) of the whole aorta, not only of the true lumen, which allowed effective use of the modified Stabilize technique. This involves ballooning the proximal and middle, but not distal, stent graft segments of the FET prosthesis to relaminate the thoracic aortic dissection membranes just below the distal anastomosis. This allows for effective and immediate mechanical haemostasis at the anastomosis “collar” of the FET prosthesis. This technique not only stops retrograde blood flow from the false lumen, but avoids distal re-dissection below the stent graft (called: stent-induced new re-entry; SINE).
In a few cases (n = 2), the decision was made to reverse the order of procedures (BEVAR before FET). Although the overall results were good in these cases, this procedure is atypical or even inconsistent with current recommendations and requires a team qualification followed by consistent staged treatment.
In 4 cases, the possibility of immediate assessment of the visceral segment and the performance of a PETTICOAT procedure (TEVAR plus BMS to the visceral aorta) allowed opening of the inflow to the mesenteric artery and renal arteries in patients after a Bentall operation performed in acute type A dissection.
Discussion
What was achieved through cooperation?
In addition to effective staged treatment, acceptable clinical results and the successful introduction of innovative technical solutions mentioned above, the most significant benefits were the so-called soft benefits for both vascular and cardiac surgeons (Table I, Figure 2).
Table I
Benefits of collaboration within the “Aortic Team”
Figure 2
Here is an example of a successfully performed staged treatment in a patient with TAAD. A – 1st stage: Successful Bentall operation after despite SCA and ROSC, B – 2nd stage: fTEVAR – PMEG in a patient with distal anastomotic tear using modified ETAG technique due to mechanical aortic valve. C – 3rd stage: BEVAR: T-Branch due to degenerative dissection in thoracoabdominal segment
Financial results
The financial result of the Aortic Team’s operation is also significant. Endovascular operations using stent grafts are generally expensive and multistage. However, in Polish conditions they are well valued by AOTMiT (Agencja Oceny Technologii Medycznych i Taryfikacji) and can be sold from the so-called “cardiac surgery code”. Therefore, the final financial result of staged treatment is definitely positive (however, we cannot provide detailed data due to data protection in force at our hospital). As a result, the establishment of the Aortic Team in Szczecin has definitely increased the profitability of hospital treatment.
Organisational structure of the “Aortic Team”
Aortic Teams should consist of vascular surgeons and cardiac surgeons experienced in advanced aortic procedures, jointly planning staged treatment based on angiotomography and performing both endovascular and open procedures. During advanced aortic procedures, as many as three doctors may be needed at the same time. Interventional cardiologists are involved in selected stages of the procedure (applies to selected types of surgery) and experienced in pre- and post-operative management and performing intraoperative trans-esophageal echocardiography (TEE). Anaesthesiologists who understand the differences in the anaesthetic management and postoperative care of major endovascular procedures and associated complications including paraplegia.
Logistics and coordination of the “Aortic Team”
It is much more complicated due to the work with individualized technical equipment and inconsistent task schedules of doctors of different specialties, who are generally employed in different departments. The delivery time of technical equipment (mainly customised stent grafts) is variable and depends on the design and production capabilities of the equipment supplier and on variable international transport conditions. This process requires dynamic tracking and adaptation of operational lists to the current availability of technical resources. The treatments are multi-stage and require planning for at least several emergency solutions (bail-outs) at each stage, which in turn requires securing the availability of technical assets that should be stored within e.g. a depot. Treatments often require the creation of individual “flow-charts” and “check lists”, concerning both equipment and key stages of the operation. The availability of these resources must be controlled on a patient-by-patient basis, rather than by a standard hospital supply mechanism. The nature of endovascular treatment means that contact with patients must be much more frequent both before and after surgery. Follow-up after the procedure follows a pattern (1, 6, 12 months, etc.) and the essence of this is angio-tomographs, which must be requested, followed up, and the studies provided to the surgical team for evaluation. This is necessary because endovascular procedures are much more likely to require re-interventions and corrections that should not be delayed (type I or III leaks). Since doctors of different specialties should collaborate in the Aortic Team, their task schedules should be taken into account when planning the work of the Aortic Team (dates of operation slots, qualification and consultation meetings). Such complex logistics, like in the case of transplant teams, require the involvement of at least one additional coordinator who is familiar with endovascular equipment and closely cooperates with the hospital Purchasing Department and providers of technical means. Supervision and coordination are also required for “online work”, which largely supports (but does not yet completely replace) the process of consultation, qualification and treatment planning for patients treated by the Aortic Team. The coordinator is also responsible for the correct settlement and reporting of treatment results of staged procedures. As these procedures often require individual settlements with the NFZ (Narodowy Fundusz Zdrowia; National Health Fund), the coordinator’s tasks also include obtaining various approvals and preparing reports for the relevant hospital “controlling” units.
What is the future of cardiac surgery?
Endovascular procedures in any segment of the aorta are significantly less invasive and carry a significantly lower risk of complications and mortality than open procedures. They are therefore chosen more frequently by both doctors and patients. Therefore, surgeons must have them in their “armamentarium” and constantly expand their experience in this field. Technological development in the treatment of stent grafts is proceeding at an explosive speed. Endovascular treatment of the aortic arch is already a reality, not to mention trans-arterial aortic valve implantation (TAVI). Treatment of the ascending aorta with an aortic valve is ongoing (the first endo-Bentall has already been performed) [8]. Endovascular mitral valve replacement has also become a fact. Operations in all these regions will naturally be displaced by endovascular technology exactly as percutaneous transluminal coronary angioplasty (PTCA) replaces coronary artery bypass graft (CABG). Therefore, as a cardiac surgeon, we suggest with some caution that it is probably time for a so-called “paradigm shift” in the approach to cardiac surgery in Poland.